Cholera worldwide overview
Monthly update as of 27 July 2026
Since 22 June 2026 and as of 27 July 2026, 8 247 new cholera cases, including 326 new deaths, have been reported worldwide.
New cases have been reported from Afghanistan, Angola, Burundi, Cameroon, Central African Republic, Chad, Democratic Republic of the Congo, Haiti, Kenya, Malawi, Mozambique, Myanmar/Burma, Pakistan, Somalia, Sudan and Yemen.
The five countries reporting most cases are Democratic Republic of the Congo (3 841), Sudan (1 502), Somalia (962), Central African Republic (445) and Malawi (383).
New deaths have been reported from Afghanistan, Angola, Burundi, Cameroon, Central African Republic, Chad, Democratic Republic of the Congo, Haiti, Mozambique, Sudan and Yemen.
The five countries reporting most new deaths are Sudan (153), Democratic Republic of the Congo (105), Central African Republic (36), Angola (12) and Cameroon (12).
In addition, 18 253 new cases were reported or collected retrospectively from before 22 June 2026.
In the previous reporting period (26 May to 22 June 2026), 19 659 new cholera cases, including 261 new deaths, were reported worldwide.
Since 1 January 2026 and as of 27 July 2026, 132 313 cholera cases, including 1 556 deaths, have been reported worldwide.
In comparison, since 1 January 2025 and as of 27 July 2025, 306 615 cholera cases, including 3 752 deaths, were reported worldwide.
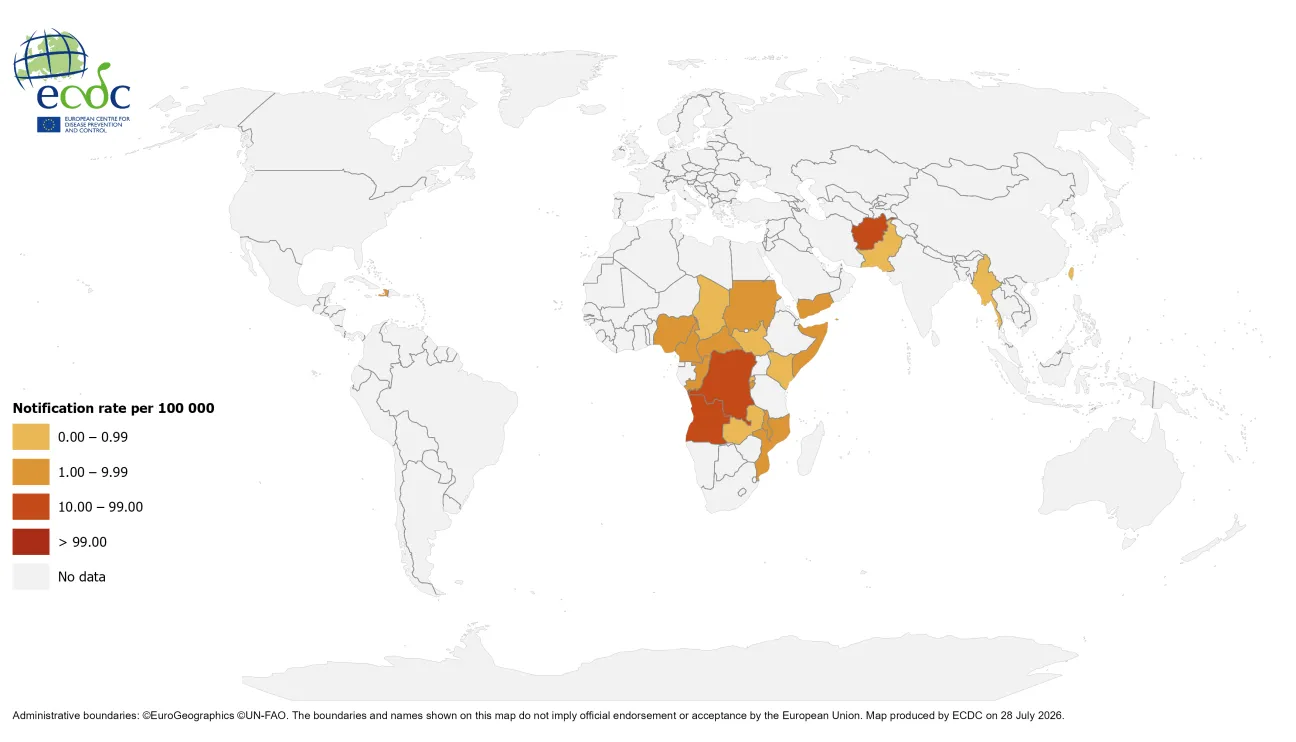
Geographical distribution of cholera cases reported worldwide from May to July 2026
Since the last update, new cases and new deaths have been reported from:
Asia:
Afghanistan: Since 18 May 2026 and as of 15 June 2026, 16 577 new cases, including 12 new deaths have been reported. Since 01 January 2026 and as of 15 June 2026, 56 662 cases, including 28 deaths have been reported. In comparison, in 2025 and as of 23 June 2025, 68 031 cases, including 26 deaths were reported.
Myanmar/Burma: Since 06 April 2026 and as of 15 June 2026, 106 new cases have been reported. Since 1 January 2026 and as of 15 June 2026, 257 cases have been reported. In comparison, in 2025 and as of 16 June 2025, 1 888 cases were reported.
Pakistan: Since 20 April 2026 and as of 18 May 2026, 701 new cases have been reported. Since 1 January 2026 and as of 18 May 2026, 3 305 cases have been reported. In comparison, in 2025 and as of 21 July 2025, 14 760 cases were reported.
Taiwan: Since 09 July 2023 and as of 19 June 2026, 1 new case has been reported. Since 1 January 2026 and as of 19 June 2026, one case has been reported. In comparison, in 2025 and as of 27 July 2025, no cases were reported. This case was briefly described in the previous monthly report.
Yemen: Since 04 May 2026 and as of 08 June 2026, 696 new cases, including one new death, has been reported. Since 1 January 2026 and as of 08 June 2026, 5 054 cases, including seven deaths, have been reported. In comparison, in 2025 and as of 23 June 2025, 41 510 cases, including 129 deaths, were reported.
Since 22 June 2026, no updates have been reported by: India.
Africa:
Angola: Since 14 June 2026 and as of 12 July 2026, 303 new cases, including 12 new deaths, have been reported. Since 1 January 2026 and as of 12 July 2026, 5 379 cases, including 116 deaths, have been reported. In comparison, in 2025 and as of 08 July 2025, 27 008 cases, including 756 deaths were reported.
Burundi: Since 14 June 2026 and as of 12 July 2026, 165 new cases, including one new death, have been reported. Since 1 January 2026 and as of 12 July 2026, 1 538 cases, including four deaths, have been reported. In comparison, in 2025 and as of 08 July 2025, 217 cases were reported.
Cameroon: Since 31 December 2025 and as of 12 July 2026, 331 new cases, including 12 new deaths, have been reported. Since 1 January 2026 and as of 12 July 2026, 331 cases, including 12 deaths, have been reported. In comparison, in 2025 and as of 27 July 2025, no cases were reported.
Central African Republic: Since 1 November 2016 and as of 9 July 2026, 445 new cases, including 36 new deaths, have been reported. Since 1 January 2026 and as of 9 July 2026, 445 cases, including 36 deaths, have been reported. In comparison, in 2025 and as of 27 July 2025, no cases were reported.
Chad: Since 31 December 2025 and as of 12 July 2026, 120 new cases, including four new deaths, have been reported. Since 1 January 2026 and as of 12 July 2026, 120 cases, including four deaths, have been reported. In comparison, in 2025 and as of 27 July 2025, no cases were reported.
Democratic Republic of the Congo: Since 14 June 2026 and as of 12 July 2026, 3 841 new cases, including 105 new deaths, have been reported. Since 1 January 2026 and as of 12 July 2026, 33 182 cases, including 943 deaths, have been reported. In comparison, in 2025 and as of 8 July 2025, 32 456 cases, including 737 deaths, were reported.
Kenya: Since 14 June 2026 and as of 12 July 2026, two new cases have been reported. Since 1 January 2026 and as of 12 July 2026, 39 cases have been reported. In comparison, in 2025 and as of 30 April 2025, 125 cases, including six deaths, were reported.
Malawi: Since 14 June 2026 and as of 12 July 2026, 383 new cases have been reported. Since 1 January 2026 and as of 12 July 2026, 2 998 cases, including five deaths, have been reported. In comparison, in 2025 and as of 7 April 2025, 91 cases, including three deaths, were reported.
Mozambique: Since 14 June 2026 and as of 12 July 2026, 193 new cases, including three new deaths, have been reported. Since 1 January 2026 and as of 12 July 2026, 7 379 cases, including 64 deaths, have been reported. In comparison, in 2025 and as of 8 July 2025, 3 832 cases, including 41 deaths, were reported.
Somalia: Since 14 June 2026 and as of 12 July 2026, 962 new cases have been reported. Since 1 January 2026 and as of 12 July 2026, 2 168 cases have been reported. In comparison, in 2025 and as of 8 July 2025, 5 414 cases, including eight deaths, were reported.
Sudan: Since 11 January 2026 and as of 12 July 2026, 1 502 new cases, including 153 new deaths, have been reported. Since 1 January 2026 and as of 12 July 2026, 1 511 cases, including 153 deaths, have been reported. In comparison, in 2025 and as of 8 July 2025, 32 230 cases, including 774 deaths, were reported.
Since 22 June 2026, no updates have been reported by: Congo, Ethiopia, Namibia, Nigeria, Rwanda, South Sudan, United Republic of Tanzania, Zambia and Zimbabwe.
Americas:
Haiti: Since 06 April 2026 and as of 18 May 2026, 172 new cases, including one new death, have been reported. Since 1 January 2026 and as of 18 May 2026, 529 cases, including two deaths, have been reported. In comparison, in 2025 and as of 23 June 2025, 2 496 cases, including 31 deaths, were reported.
ECDC assessment:
Cholera cases have continued to be reported in Africa and Asia, the Middle East, and the Americas.
In this context, although the likelihood of cholera infection for travellers visiting these countries remains low, sporadic importation of cases to the EU/EEA is possible.
In the EU/EEA, cholera is rare and primarily associated with travel to endemic countries. Since 2025, only events of locally acquired cholera cases are reported at the EU/EEA level; however, imported and locally acquired cholera cases are reported to the World Health Organization (WHO) on an annual basis. In 2024, 16 imported cases were reported by eight EU/EEA countries, while 12 were reported in 2023, 29 in 2022, two in 2021, and none in 2020. In 2019, 25 cases were reported in EU/EEA countries (including the United Kingdom). All cases had a travel history to cholera-affected areas.
Vaccination should be considered for travellers at higher risk of infection, such as emergency and relief workers who may be directly exposed. Vaccination is generally not recommended for other travellers. Travellers to cholera-endemic areas should seek advice from travel health clinics to assess their personal risk, and apply precautionary sanitary and hygiene measures to prevent infection. Such measures can include drinking bottled water or water treated with chlorine, carefully washing fruit and vegetables with bottled or chlorinated water before consumption, regularly washing hands with soap, eating thoroughly cooked food, and avoiding the consumption of raw seafood products.
Actions:
ECDC continues to monitor cholera outbreaks globally through its epidemic intelligence activities in order to identify significant changes in epidemiology and provide timely updates to public health authorities.
Reports are published on a monthly basis. The worldwide overview of cholera outbreaks is available on ECDC's website.
Read more
All updates on cholera

Cholera is an acute diarrhoeal infection caused by the bacterium Vibrio cholera of serogroups O1 or O139. Humans are the only relevant reservoir, even though Vibrios can survive for a long time in coastal waters contaminated by human excreta.