Epidemiological update: Diphtheria cases in Europe
Since January 2022, and as of 11 August 2023, 281 confirmed diphtheria cases, as per the EU case definition (2022: 224 cases, 2023: 57 cases), and four deaths were reported in the EU/EEA through the European Surveillance System (TESSy), compared to an average of 55 cases reported annually between 2017 and 2021.
During late summer 2022, intelligence data reported to ECDC indicated that the majority of cases in 2022 were diagnosed in migrant-related facilities, with onward transmission documented in a few instances in migrant-related-facilities (see Eurosurveillance article on cases in Germany and Switzerland). ECDC is not aware of any evidence indicating outbreaks in the broader EU/EEA population resulting from the cases identified in these settings.
The 281 cases were reported by Germany (206), Belgium (37), Czechia (10), Slovakia (9), Netherlands (9), Sweden (5), Latvia (3), Norway (1) and Spain (1). The two deaths reported in 2023 occurred in Belgium and Latvia. In 2022, one death was reported in Germany and one in Slovakia. The age range of cases was between 0 and 92 years with 175 cases (62%) in the age group 15– 5 years, with 240 (85%) being male. Overall, 228 cases were caused by Corynebacterium (C.) diphtheriae and 53 cases were caused by Corynebacterium (C.) ulcerans. Of the 228 cases caused by C. diphtheriae, 199 were cutaneous, 18 respiratory, three had both a cutaneous and respiratory presentation and three had a nasal presentation. Five cases had a different clinical manifestation or missed information about the clinical manifestation. Of the fatal cases, three were attributable to C. diphtheriae infections and one was attributable to C. ulcerans. Two of the fatal cases presented with respiratory disease, one with cutaneous disease and one with a different clinical presentation.
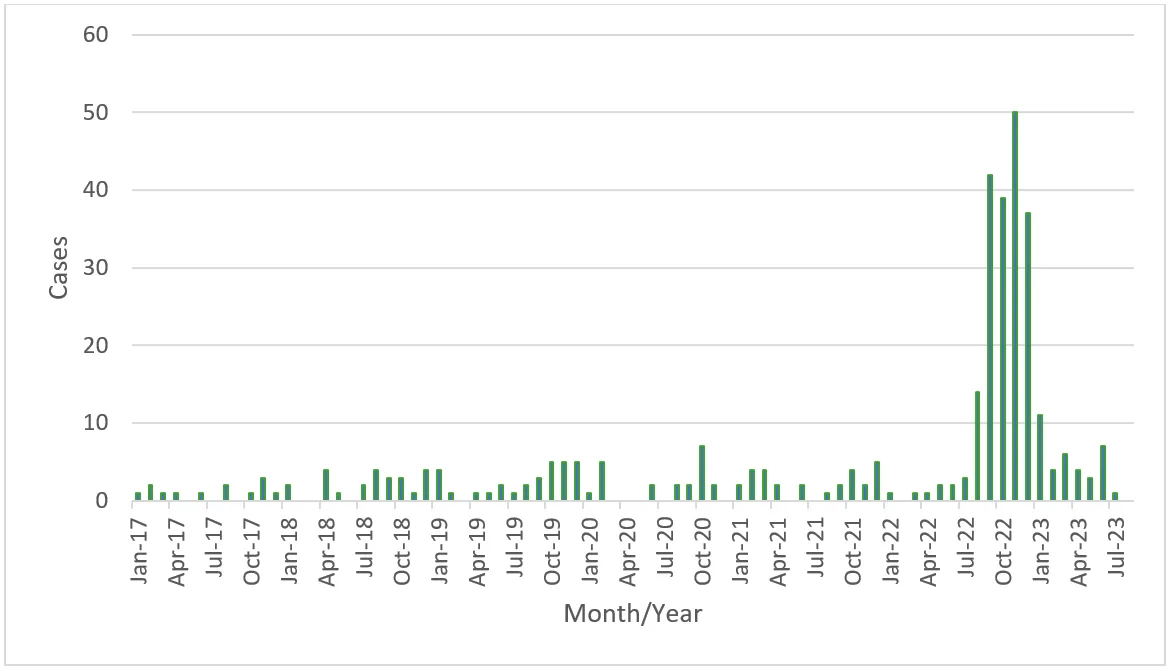
Figure 1. Number of C. diphtheriae cases reported to ECDC via TESSy, and month/year, 1 January 2017-11 August 2023
Microbiological aspects of selected cases of diphtheria in migrants 2022 and 2023
Following the increased numbers of diphtheria cases reported at the EU level and in addition to increased efforts to contain the outbreak, a pan-European consortium was set up to provide further insight on the microbiological profile of the cases reported in migrant-related facilities, focusing on the period between 1 January and 30 November 2022. The consortium retrospectively identified a total of 363 isolates of tox-gene-bearing C. diphtheriae from 362 individuals, with the following geographical distribution: Germany (118), Austria (66), UK (59), Switzerland (52), France (30), Belgium (21), Norway (8), The Netherlands (5), Italy (3), and Spain (1) in the study period. Of these, around 95% lived in a migrant facility, reported a recent arrival in the reporting country or had close links to migrant communities.
Most cases involved cutaneous diphtheria, although some respiratory cases and two fatalities were observed during the study period. The analysis of the genetic relatedness and antibiotic susceptibility patterns showed a simultaneous multi-country outbreak of three distinct sequence types (ST377 (n=125), ST384 (n=74) and ST574 (n=131)) with highly related isolates reported in nine of the ten countries reporting cases. One of these sequence types (ST377) also had a subcluster (n=17) that exhibited a concerning antimicrobial resistance profile to first line antibiotics (beta-lactams and macrolides) used in the treatment of diphtheria. The close genetic relatedness within clusters supports recent transmissions, most likely on the migrant route and/or within migrant facilities. Outside the study period, in 2023, consortium members observed a total of 48 cases in migrants, of which 33 of those with typing data available belong to the STs described in migrants in 2022. The isolate from the fatal case from Belgium could not be typed because of prior antibiotic treatment.
Assessment
Diphtheria is a rare disease in EU/EEA countries. According to WHO/UNICEF, immunisation coverage estimates for diphtheria, tetanus toxoid and pertussis (DTP3) in 2022 in the EU/EEA varied across Member States, ranging from 85% (Austria) to 99% (Greece, Hungary, Luxembourg, Malta and Portugal). Universal immunisation is the only effective method for preventing the toxin-mediated disease. This includes the administration of booster doses of diphtheria toxoid as per national recommendations. The occurrence of the disease in fully vaccinated individuals is very rare.
The number of cases reported to ECDC and information provided as part of the microbiological study indicate that cases of C. diphtheriae continue to be diagnosed in the EU/EEA – mainly in migrant individuals and presenting with cutaneous presentation; however the number of cases appear to be smaller in 2023 than in the second part of 2022. The observed picture among migrants needs continued attention and implementation of public health and response measures where cases are identified, also considering the observed presence of antimicrobial resistance profiles that threaten the efficacy of first-line treatments, the lack of diphtheria anti-toxin (DAT) global supply and possible low clinical suspicion.
To achieve the highest levels of protection and maximise opportunities for the prevention of diphtheria diseases, EU/EEA countries are encouraged to consider a broad number of actions which include:
- Increase awareness of diphtheria disease as well as current epidemiology of disease in EU/EEA;
- Strengthen the implementation of routine immunisation programmes, seeking to achieve high vaccination coverage rates with the primary series of three doses of the diphtheria toxoid-containing vaccine, followed by booster doses;
- Implement systems, including the use of immunisation information systems, to identify and reach out to the unvaccinated or partially vaccinated population with a primary immunisation series and/or booster doses;
- Ensure the provision of booster doses to the adult and elderly population, considering waning protection from the primary series. Checking immunisation status at key healthcare encounters and vaccinating, when necessary, could be an effective mechanism to better integrate immunisation efforts as part of healthcare delivery services and promote optimal uptake;
- Promote and monitor equity of access to immunisation. This applies particularly to vulnerable populations or population groups at risk of being socially marginalised, such as migrants, refugees and asylum seekers. These groups may be entering the EU/EEA being insufficiently immunised due to interruption in their immunisation programme as a consequence of war or social unrest. Vaccination against priority diseases such as diphtheria, poliomyelitis and measles, which are particularly prone to spread in crowded areas and settings such as refugee centres, should be offered promptly to children, adolescents, and adults alike. In the absence of documentation of prior vaccination, vaccination should be offered promptly.
ECDC encourages EU/EEA countries to timely report confirmed cases to TESSy, aiming at a high level of completeness. The timely collection and sharing of sequencing data combined with epidemiological information can support generating hypotheses on where transmission has occurred, including supporting identification of potential secondary cases in the EU/EEA population. On a needs basis, ECDC can support member states in the sequencing and molecular typing of C. diphtheriae. Please contact typing ecdc [dot] europa [dot] eu (typing[at]ecdc[dot]europa[dot]eu) for further details.
ecdc [dot] europa [dot] eu (typing[at]ecdc[dot]europa[dot]eu) for further details.
More information




Share this page