Epidemiological update: Middle East respiratory syndrome coronavirus (MERS-CoV)
Since April 2012 and as of 4 June 2014, 815 cases of MERS-CoV infection have been reported by local health authorities worldwide, including 313 deaths.
Since April 2012 and as of 4 June 2014, 815 cases of MERS-CoV infection have been reported by local health authorities worldwide, including 313 deaths.
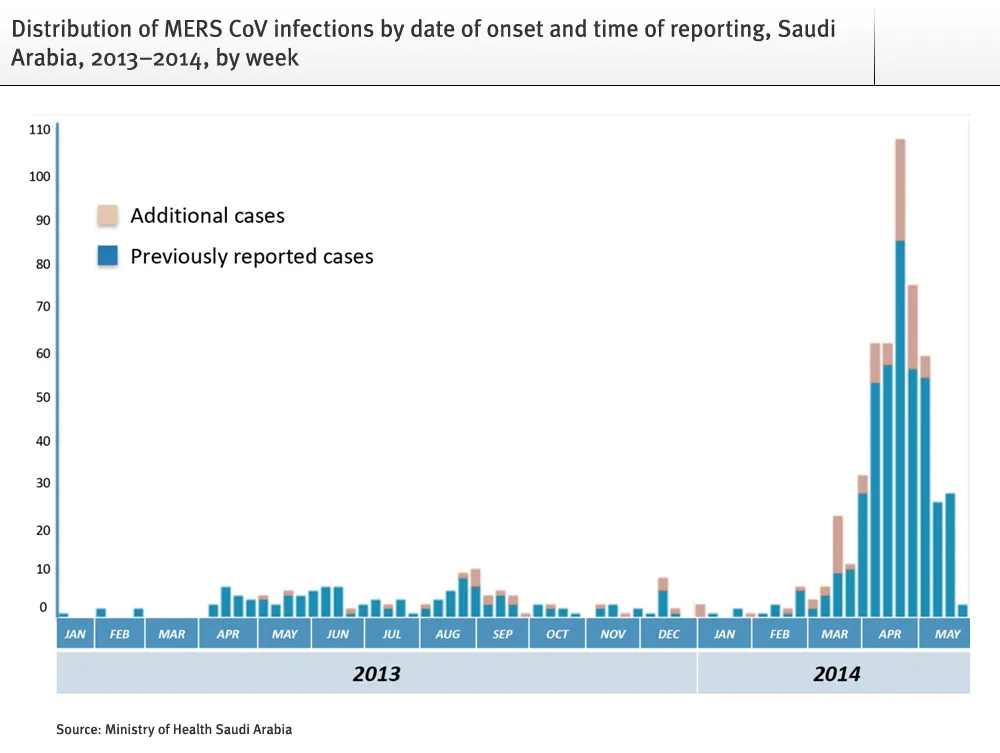
On 3 June 2014, the Ministry of Health of Saudi Arabia updated the MERS case count with 113 previously unreported cases representing a 20% increase in the cumulative number of cases. The number of cases is 688 of which 353 have recovered, 282 have died and 53 are receiving care. These new cases have been retrospectively identified during a review of the data. Ninety-two of the 113 cases reported on 3 June were fatal, increasing the number of deaths from MERS-CoV in Saudi Arabia by 48% from 190 to 282, and raising the case-fatality ratio (CFR) from 33% to 41%. The retrospectively identified newly reported cases date back to May 2013. Information about age, gender, residence, probable place of infection, whether the case is sporadic/primary or part of a cluster of secondary transmission, health care associated transmission or not, and whether the case is a healthcare worker, is missing for these retrospectively reported cases. In addition, it is unclear whether these cases are meeting the WHO case definition for confirmed cases.
The MOH also announced new measures to improve the capacity and efficiency of Saudi laboratories and testing facilities.
Figure 1.
On 27 May 2014, the Iranian health authorities reported two cases involving two middle-aged sisters, without travel history, but with contact with a person, who had influenza-like illness symptoms after travel to Saudi Arabia. One of the sisters has died.
On 31 May 2014 the Algerian health authorities reported two cases in middle aged men, who both had recent travel history to Saudi Arabia for performing Umrah.
Table 1. Confirmed cases, deaths and date of onset for the most recent case, by region as of 4 June 2014
| Region/country | Cases | Deaths | Date of onset for most recent case |
| Middle East | |||
| Saudi Arabia | 689 | 283 | 28/05/2014 |
| United Arab Emirates | 70 | 9 | 04/05/2014 |
| Qatar | 7 | 4 | 04/11/2013 |
| Jordan | 18 | 5 | 23/05/2014 |
| Oman | 2 | 2 | 20/12/2013 |
| Kuwait | 3 | 1 | 07/11/2013 |
| Egypt | 1 | 0 | 22/04/2014 |
| Yemen | 1 | 1 | 17/03/2014 |
| Lebanon | 1 | 0 | 22/04/2012 |
| Iran | 2 | 1 | 27/05/2014 |
| Europe | |||
| UK | 4 | 3 | 06/02/2013 |
| Germany | 2 | 1 | 08/03/2013 |
| France | 2 | 1 | 08/05/2013 |
| Italy | 1 | 0 | 31/05/2013 |
| Greece | 1 | 0 | 08/04/2014 |
| Netherlands | 2 | 0 | 05/05/2014 |
| Africa | |||
| Tunisia | 3 | 1 | 01/05/2013 |
| Algeria | 2 | 0 | 24/05/2014 |
| Asia | |||
| Malaysia | 1 | 1 | 08/04/2014 |
| Philippines | 1 | 0 | 11/04/2014 |
| Americas | |||
| USA | 2 | 0 | 01/05/2014 |
| Total | 815 | 313 |
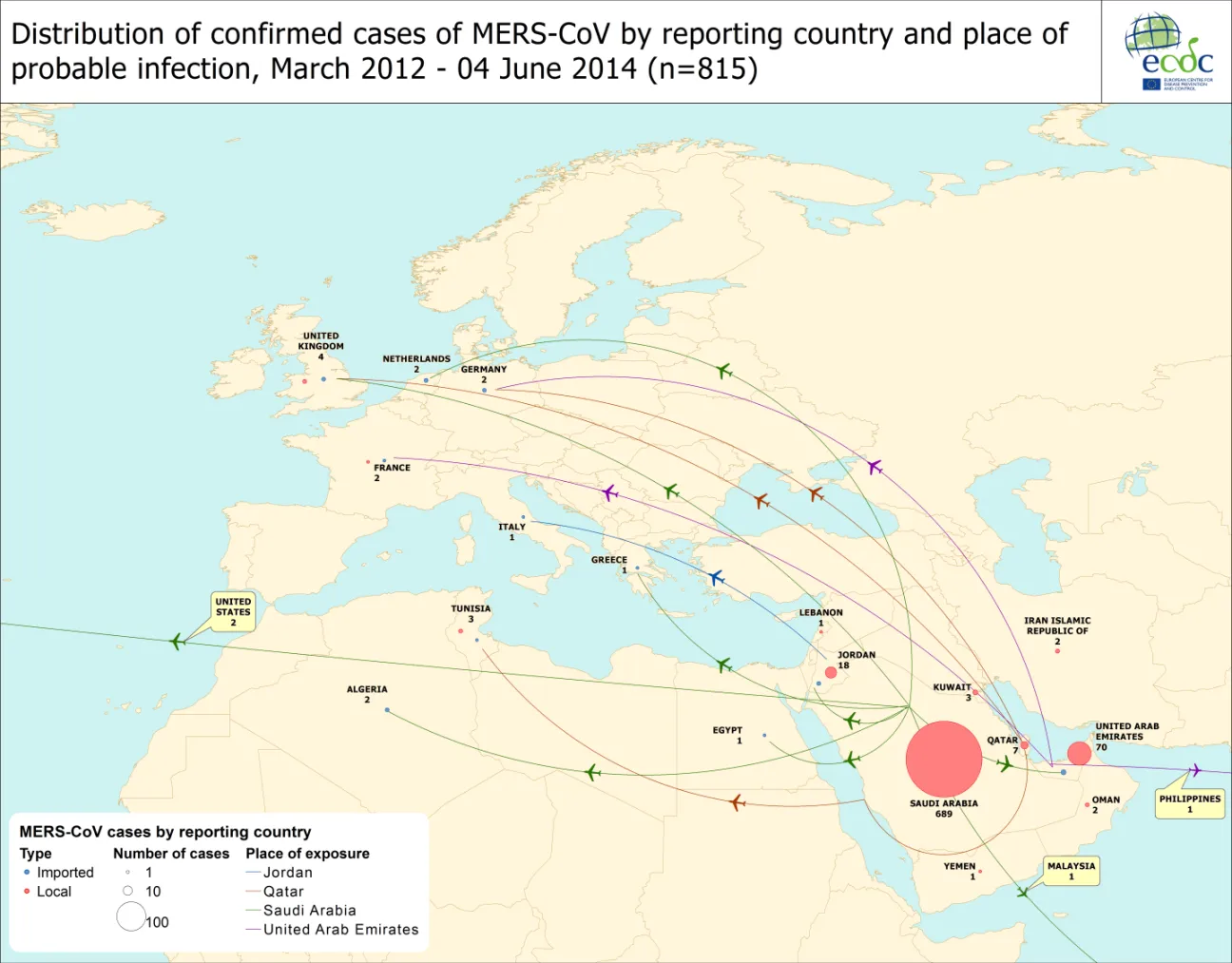
Twenty-one cases have been reported from outside the Middle East. In France, Tunisia, the UK, and Iran, there has been local transmission to people who had not travelled to the Middle East, but had been in close contact with laboratory-confirmed or probable cases. Person-to-person transmission has occurred both among family contacts and in healthcare facilities.
All cases have either occurred in the Middle East or have direct links to a primary case infected in the Middle East.
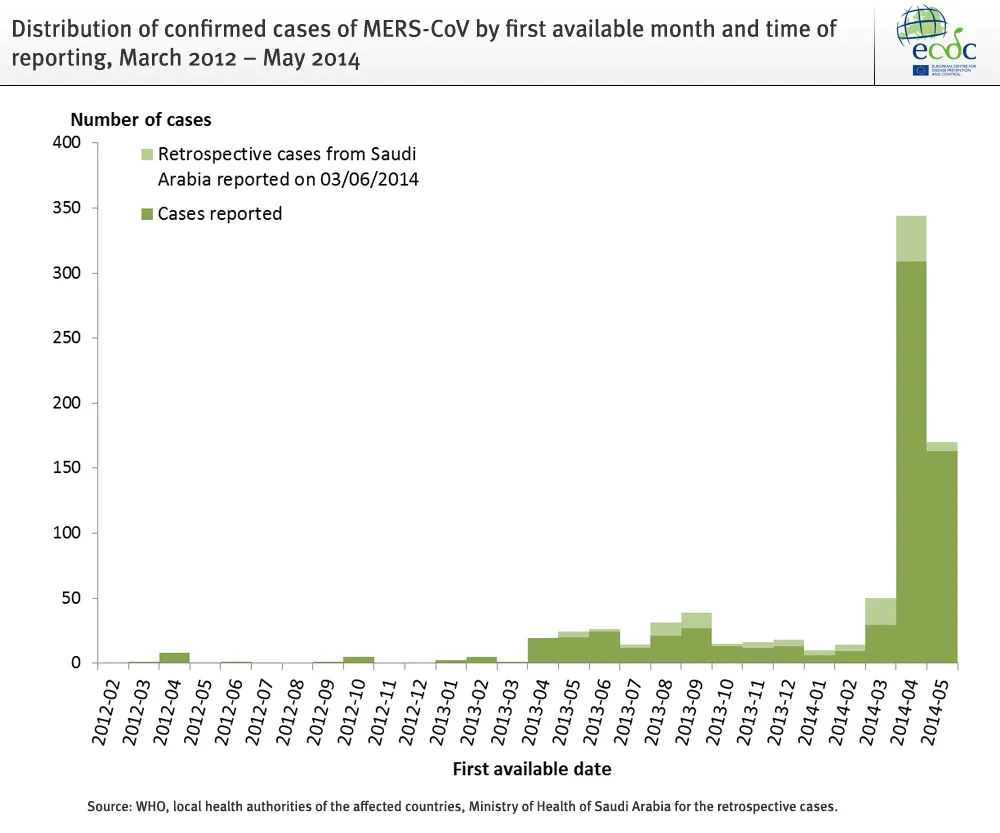
Figure 2.
In May 2014, two new countries, Iran and Algeria, reported cases (Figure 3).
Figure 3.
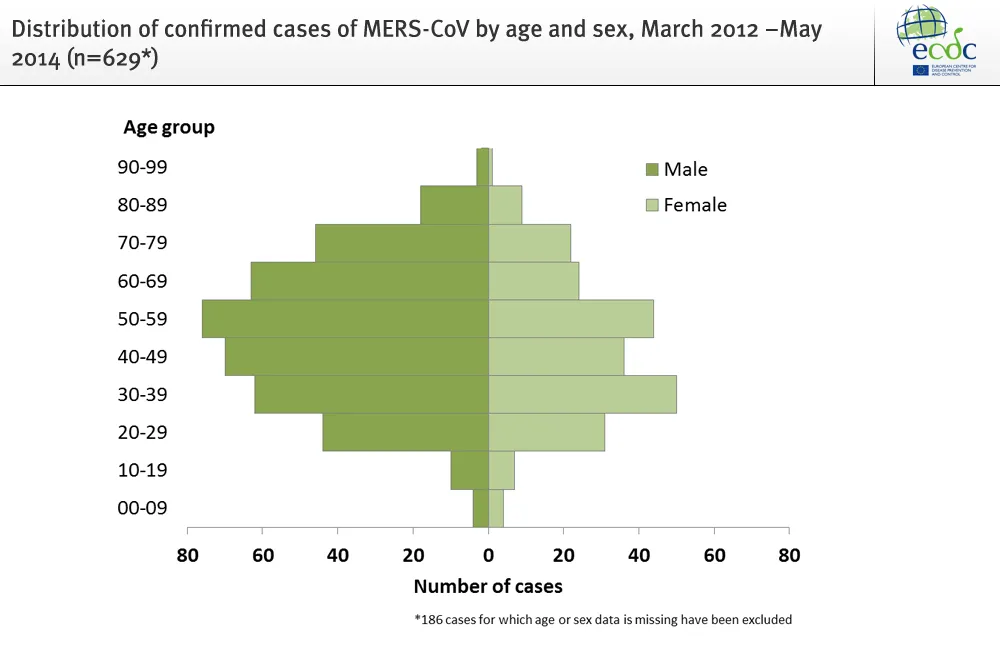
As of 4 June 2014, overall, the case-fatality-ratio is 38%. Of the 629 cases the male to female ratio is 1.7:1. The majority of the cases 275 (44%) are among men older than 40 years.
Figure 4.
ECDC continues to monitor information on the situation on MERS-CoV worldwide. In earlier Rapid Risk Assessments, ECDC concluded that the risk of importation of MERS-CoV to the EU was expected to continue and the risk of secondary transmission in the EU remains low. The conclusions of the assessment provided in the ECDC rapid risk assessment (RRA) remains valid.
Conclusions
The cases and fatalities reported in batch by Saudi Arabia on 3 June improves the completeness of data but does not significantly change the epidemiological pattern of the outbreak. The new cases have resulted in an increase in the case-fatality ratio, indicating that the observed trend of falling CFR over time can to some extent be explained by incompleteness of data and failure to report outcomes for already notified cases. The new information does not change the ECDC risk assessment of 31 May 2014.


