ECDC classifies XBB.1.5-like lineages with the amino acid change F456L as variants of interest following an increase in SARS-CoV-2 transmission in EU/EEA countries and abroad
In 2023, after several months of very low rates of infection, coronavirus disease 2019 (COVID-19) transmission has started to increase in some EU/EEA countries. Although this has coincided with increasing detections of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) XBB.1.5-like lineages carrying the F456L mutation, there are other drivers that can contribute to the increasing transmission rates. This includes large gatherings during seasonal holidays and lower levels of immunological protection against infection after several months of very low disease incidence. There is currently no sign of increased hospitalisations or pressures on healthcare systems.
ECDC classified XBB.1.5-like lineages with the additional amino acid change F456L as variants of interest (VOI) due to a rapid increase in the proportion of these variants presently in circulation, which may have immune-escape properties compared to the variants which were previously in circulation.
Based on what is observed in countries outside the EU/EEA, it is likely that F456L variants will contribute to increased transmission in the coming weeks. However, it is unlikely that the resultant levels of severe disease will reach those of similar peaks previously observed during the COVID-19 pandemic. It is also unlikely that F456L variants are associated with any increase in infection severity compared to the previously circulating variants, or reduction in vaccine effectiveness against severe disease. However, as for other SARS-CoV-2 variants, older individuals and those with underlying conditions could develop severe symptoms if infected.
The completeness and timeliness of epidemiological and virological COVID-19 surveillance data has decreased in the last year, which affects the ability to make an assessment for all EU/EEA countries. Member States are encouraged to expand their use of, and report data from well-designed, representative population-based surveillance in primary and secondary care to monitor trends in transmission and severe disease by time, place, and person, in a timely manner. Where possible, all SARS-CoV-2-positive specimens from representative surveillance systems should be sequenced and reported to the Global Initiative on Sharing All Influenza Data (GISAID) and/or The European Surveillance System (TESSy) to facilitate the assessment of circulating variants.
Adherence to national vaccination schedules is essential to protect people at high risk for severe disease and death. Countries should assess their readiness to identify target groups and conduct timely COVID-19 vaccination campaigns. In addition, communication campaigns aimed at the public and healthcare professionals are deemed necessary to reach high-risk groups and inform them of the importance to stay up to date with vaccination.
XBB.1.5-like + F456L variant
As of 10 August 2023, ECDC classified all XBB.1.5-like lineages with the additional spike protein change F456L as SARS-CoV-2 variants of interest (VOI). The reasons for this classification are: a) the rapid increase in the proportion of this mutation in the positive samples from EU/EEA countries, b) a slight increase in the epidemiological indicators of community transmission, and c) the mutation is predicted and verified by a preliminary in-vitro study to contribute to immune escape, compared to the previously circulating variants [1].
So far there is no evidence that F456L variants meet any of the criteria for variants of concern (VOC), i.e. moderate to high evidence of the variant being associated with an increase in infection severity, a risk for compromising the healthcare capacity in the EU/EEA, or a reduction in vaccine effectiveness (Figure 1). ECDC SARS-CoV-2 variant classification criteria and recommended actions for EU/EEA Member States are outlined on the ECDC variant webpage [2,3].
Figure 1. Variant classification matrix for variants of interest (VOI): XBB.1.5-like + F456L
|
ECDC criteria as of 29 June 2023 |
VUM |
VOI |
VOC |
|---|---|---|---|
| Genetic changes predicted/known to impact virus characteristics: transmissibility, virulence, immune evasion, therapeutics, detectability |
Yes | Yes | Yes |
|
(Weak) |
(Low-Mod) |
(Mod-High) |
|
Predicted growth advantage in the EU/EEA |
Yes |
Yes |
Yes |
|
Predicted EU/EEA epi impact (increases in cases or other measure) |
Unclear |
Possible |
Likely |
|
ECDC risk assessment to be undertaken |
No |
Yes |
Yes |
|
Risk assessment confirms with moderate/high certainty any of - increased severity - risk of healthcare system compromise - reduced vaccine effectiveness |
N/A |
No |
Yes |
VUM: variants under monitoring; VOI: variants of interest; VOC: variants of concern
The mutation is also increasing globally, with the World Health Organization (WHO) classifying EG.5, which is the most prevalent lineage with this mutation, as a VOI as of 9 August 2023 [4] and the United Kingdom Health Security Agency (UKHSA) classifying EG.5.1 as a variant as of 31 July 2023 [5]. ECDC classifies EG.5 within the group of lineages carrying F456L, since all 456L-lineages exhibit elevated growth rates, and the likely source of the elevated growth rate is mainly the F456L change itself.
The XBB.1.5-like lineages with F456L are characterised by spike protein receptor-binding domain changes F456L, N460K, S486P, and F490S. The XBB.1.5-like umbrella already comprises several distinct lineages which are all descendants from the recombinant lineage XBB that emerged and became successful in late 2022. Among these, there are XBB.1.5, XBB.1.9.1, XBB.1.9.2, XBB.1.16, and XBB.2.3. Several different sub-lineages within these have now acquired the additional spike protein change F456L which currently seems to confer a selective advantage over the previously circulating variants. Among these lineages, there is FE.1, which rose to high proportions close to dominance in Brazil in May 2023, but did not have wider success globally. There is also EG.5, which is now the most common lineage within the F456L group, both globally and in the EU/EEA (Figure 2).
Figure 2. Distribution of the lineages assigned within XBB.1.5-like + F456L, per sample collection week (globally) as of 14 August 2023
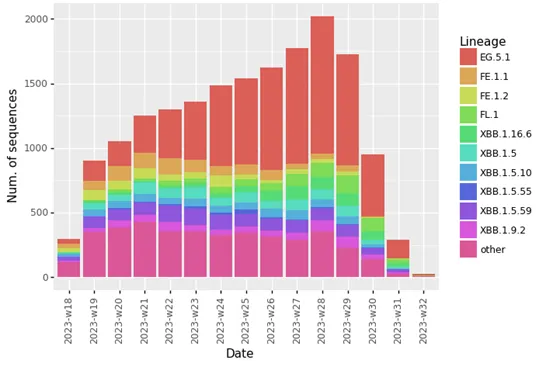
Source: GISAID EpiCoV (Note, that the assignment of novel lineages in GISAID EpiCoV is associated with some delay. For this reason, some sequences are assigned to more parental lineages. Reporting delays affect the number of sequences from the last three to four weeks shown in the figure.)
The CoV-spectrum tool provides estimates of the weekly growth advantage of variants over the currently circulating variants using a logistic regression model fitted to data from GISAID EpiCoV. These estimates are associated with significant uncertainty due to potential biases in the underlying data.
As of 14 August 2023, the EG.5 lineage is estimated to have a weekly growth advantage relative to the previously circulating lineages in the United States – US (1.38), the UK (1.51), and Europe (1.59) [6].
Among the other lineages within the F456L group that are circulating in lower proportions (e.g. FL.1.5.1, XBB.1.16.6, and XBB.1.5.59), the FL.1.5.1 lineage is also currently estimated to have a large growth advantage relative to the previously circulating lineages in the US (1.67) and the UK (1.47) [7]. This variant is also currently the dominant lineage in the Dominican Republic (61% proportion),and is circulating in low proportions in EU/EEA countries.
The lineage XBB.1.16.6 has also been estimated to have growth advantage in the US (1.39), the UK (1.57), and Europe (1.44) [8]. The growth advantage observed for 456L-lineages is most likely caused by increased immune escape conferred by the F456L change [1], combined with waning immunity to infection in the population.
Epidemiological situation and XBB.1.5-like + F456L globally, as of 14 August 2023
The latest epidemiological bulletin of WHO reports that cases of COVID-19 globally remain at low levels in August 2023, compared with the last peak of cases in November to December 2022. Cases of COVID-19 decreased between December 2022 and June 2023, when the cases reached the lowest levels observed in 2023 [9].
Between 10 July and 6 August 2023, 1.5 million new cases of COVID-19 and over 2 500 deaths have been reported. This constitutes an increase of 80% in cases of COVID-19 compared to the previous reporting period. The number of deaths, however, decreased by 57%. During this period, 103 countries reported COVID-19 data to WHO. However, due to the global reduction in testing and reporting, number of reported cases do not reflect infection rates adequately. All the WHO Regions reported a decrease in cases of COVID-19 during this period, except the Western Pacific Region which showed an increase of 137% compared with the previous reporting period. This was mostly driven by a large increase in the number of cases in South Korea.
Outside of the EU/EEA, the following countries reported an increase in cases of COVID-19 during this period in 2023:
- Reported a moderate increase: the UK, Georgia, and Nepal;
- Reported a high increase: South Korea, Honduras, Jamaica, and the Dominican Republic.
In addition, the ECDC Epidemic Intelligence team has identified signals of increases in cases of COVID-19 through open media sources in the following countries:
- In the EU/EEA: Ireland [10], Malta [11], and Portugal [12].
- Outside the EU/EEA:
- Japan: On 4 August 2023, media reported that cases of COVID-19 had increased by 14% compared to the previous week. This increase was observed for the 17th week running. Hospital admissions increased by around 16% compared to the previous week [13].
- South Korea: Media reported on 16 August 2023 that cases of COVID-19 in South Korea had increased for the seventh consecutive week, but the rate of growth has slowed down from a peak of 35.8% in the previous three weeks to 0.8% in the latest week. The number of deaths associated with COVID-19 increased by 40.2% week-on-week, but remained at low levels (136), while the number of critically ill patients increased by 21.5% (to 215) [14].
- The UK: Media and government data reported increases in the number of cases and hospitalisations since early July 2023. COVID-19 weekly hospital admissions on 4 August 2023 (1 802) more than doubled compared with four weeks earlier (721 on 30 June 2023). Even though hospital admissions increased, they remained at low levels compared to previous peaks, e.g., in December 2022 (8 075 on 23 December 2022). There are no indications of increases in deaths. EG.5.1 accounted for between 10–17% of cases and is the second-most prevalent strain in the UK, according to the UKHSA. Some of the increase has been attributed to increased social mixing indoors during wet weather [15].
- The US: Media and the United States Centers for Disease Control and Prevention (US CDC) have reported about increases in cases of COVID-19, hospital admissions, test positivity rates, and visits to emergency department over the summer. Numbers remain relatively low though. The US CDC noted that during the past three summers, the US has experienced peaks in cases of COVID-19 in summer, so the current situation is not unexpected. Data from the US CDC indicate increases in hospitalisations by 14% in the week ending 5 August 2023 compared to the previous week. The percentage of deaths due to COVID-19 increased by 10% compared to the previous week, but remain at low levels (1.1%) [16]. EG.5 is the most commonly detected variant in the US (17.3% according to nowcasting estimates for the week ending 5 August 2023) [17,18].
Figure 3. Proportion of sequences belonging to XBB.1.5-like + F456L, per sample collection week, reported by non-EU/EEA countries to GISAID EpiCoV, as of 14 August 2023
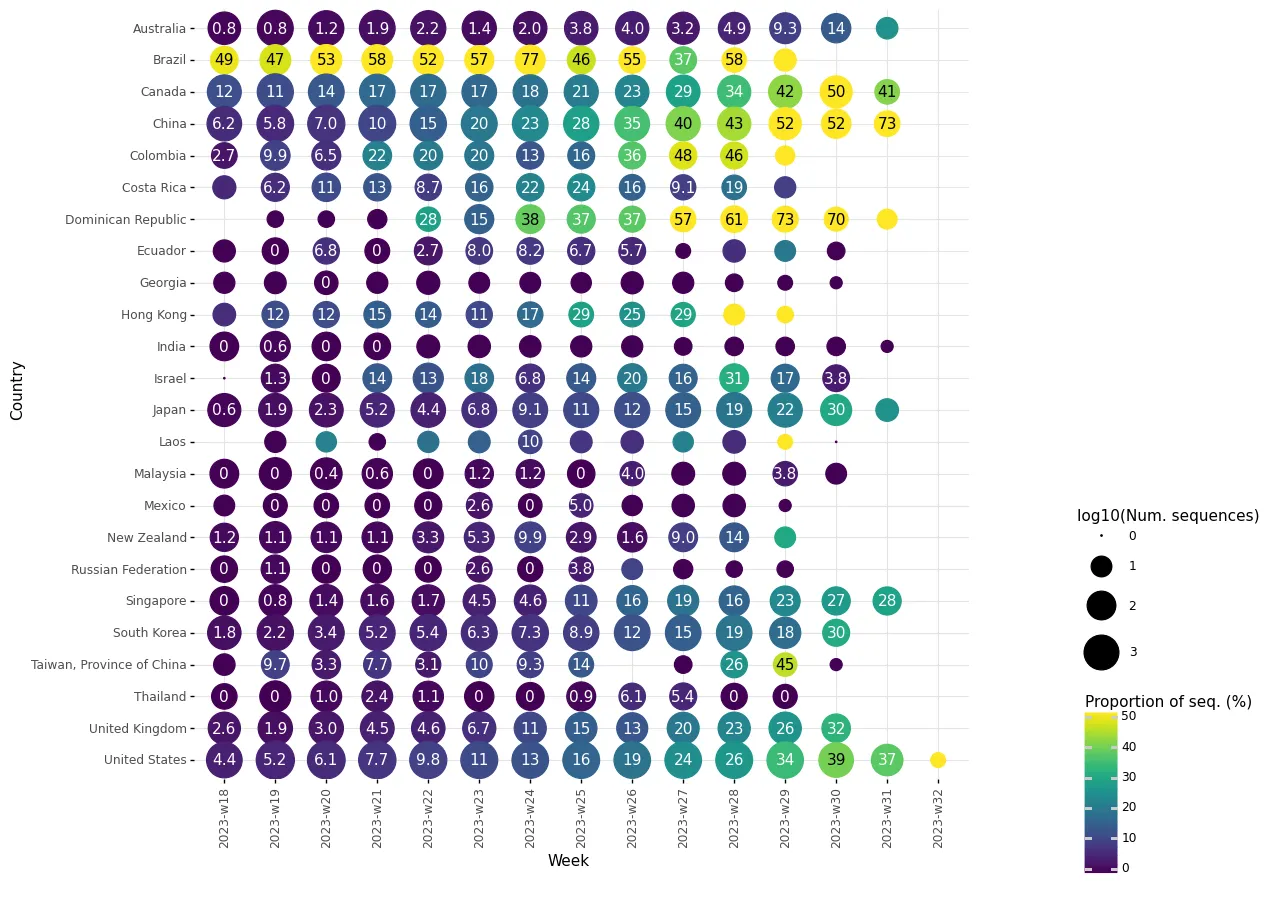
Source: GISAID EpiCoV
XBB.1.5-like + F456L in the EU/EEA, as of 14 August 2023
The nine EU/EEA countries reporting at least 10 sequences to GISAID EpiCoV for week 29 (17 July to 23 July 2023) showed the following proportions of XBB.1.5-like + F456L lineages: Denmark (41%), France (42%), Germany (10%), Iceland (59%), Ireland (47%), Italy (10%), Portugal (60%), Spain (34%), and Sweden (24%). The overall trend for the variant proportion is increasing (Figure 4). The most common lineage within XBB.1.5-like + F456L is EG.5 and its sub-lineages (Figure 5).
Figure 4. Proportion of sequences belonging to XBB.1.5-like + F456L, per sample collection week, reported by EU/EEA countries to GISAID EpiCoV as of 14 August 2023
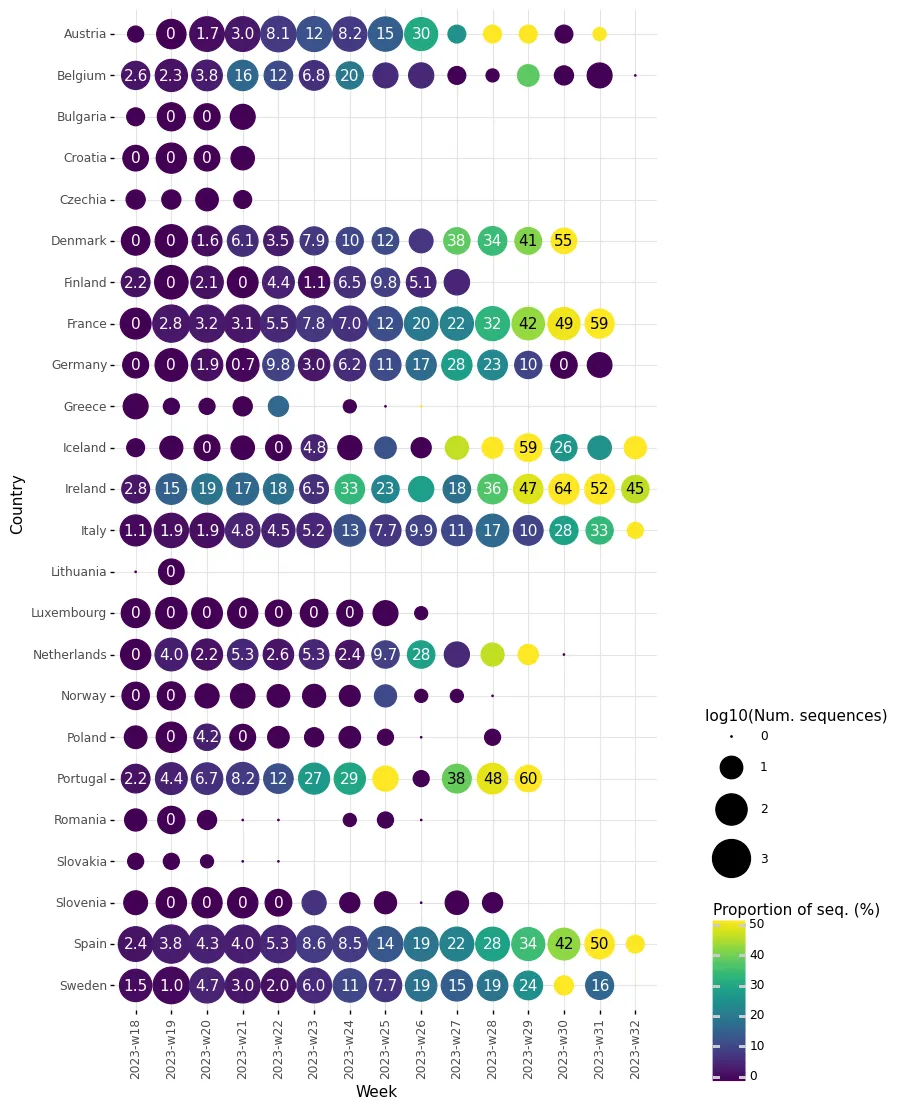
Source: GISAID EpiCoV
Figure 5. Proportion of sequences belonging to EG.5 and its sub-lineages, per sample collection week, reported by EU/EEA countries to GISAID EpiCoV, as of 14 August 2023
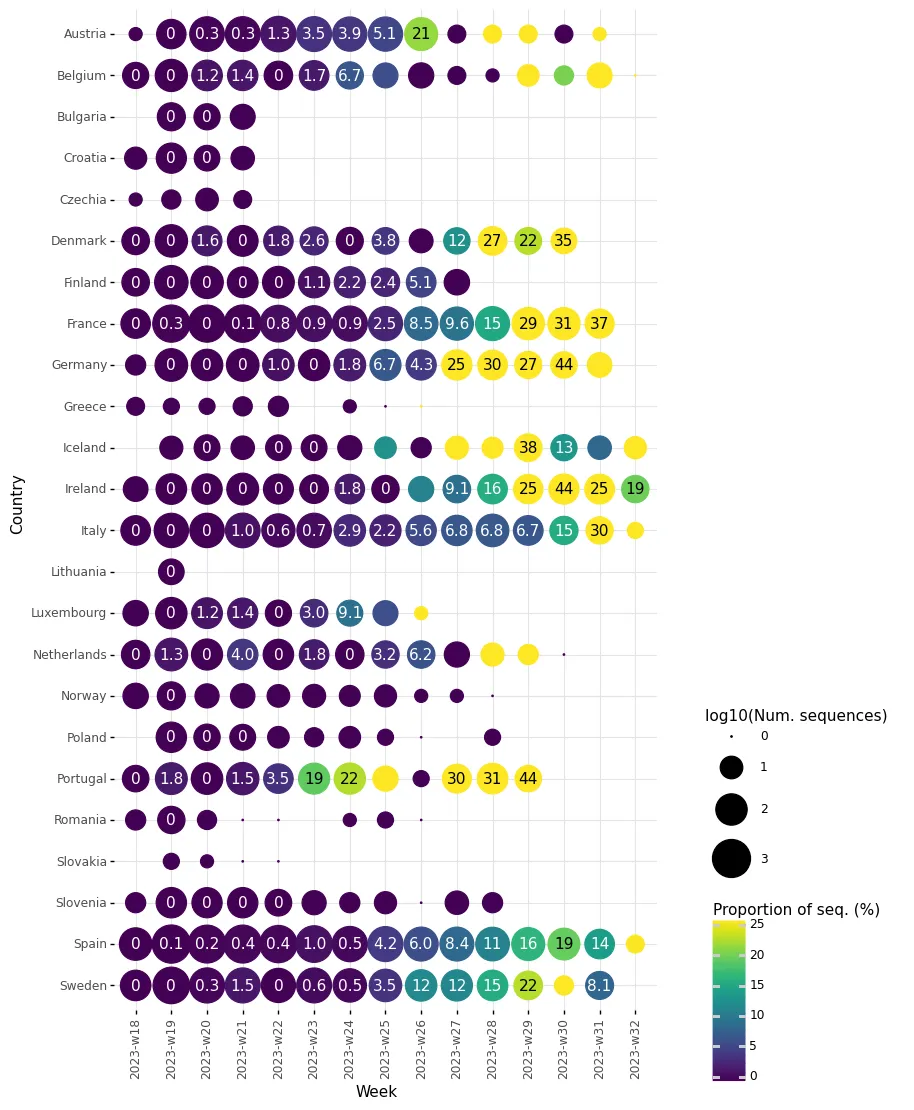
Source: GISAID EpiCoV
Sequences that are not part of the XBB.1.5-like + F456L umbrella are mainly from other XBB.1.5-like lineages, and there are also some BA.2.75-descendant lineages still in circulation, such as CH.1.1.
Epidemiological situation in the EU/EEA as of 6 August 2023
Data reported to ECDC by the end of week 31 (ending 6 August 2023) suggest that transmission of SARS-CoV-2 is increasing in many countries across the EU/EEA from the low levels observed during the summer [19]. Increasing levels of respiratory illness among patients presenting to sentinel general practitioners were reported in some countries, together with an elevated proportion of positive tests for SARS-CoV-2 in this setting. Additionally, among 18 countries which are still able to report age-specific counts of cases testing positive for COVID-19, half of them observed increases in COVID-19 case rates among people aged 65 years.
The availability of data on severe COVID-19 disease is more limited, but suggests minimal impact on severity to date. None of the four countries reporting data from severe acute respiratory infections (SARI) surveillance up to week 31 observed increasing or elevated rates of SARI hospitalisations. One additional country without a SARI surveillance system reported an increasing trend in COVID-19 hospital admissions compared to the last week. Four countries observed increasing death rates in the 65–79 years and 80 years and above age groups. These trends in reported deaths and hospital admissions are recent (of one to three weeks’ duration) and current levels remain very low relative to peaks reported during the pandemic.
Monitoring and reporting
Current data availability makes it challenging to assess the COVID-19 epidemiological situation in the EU/EEA. Although some countries have continued with primary care syndromic surveillance this summer, the low levels of testing of symptomatic patients in these settings add substantial uncertainty to estimates of SARS-CoV-2 positivity. SARI surveillance has been expanded in the EU/EEA but is still limited to relatively few countries. As of week 31, around two-thirds of countries reported data on counts of cases testing positive for COVID-19, a third reported data on admissions to hospital or ICU, and half reported data on COVID-19 deaths. These can still be a useful complement to data from sentinel systems, but must be treated with some caution. The lack of a proper case definition and potential for changes in underlying strategies for testing and reporting can introduce bias or artefact. The reduction in PCR testing and low levels of transmission over the summer has also led to very limited volumes of sequencing, which limits ECDC’s ability to assess variants.
As outlined in the guidance document, ‘Operational considerations for respiratory virus surveillance in Europe’ [19], EU/EEA Member States are encouraged to expand their use of, and report data from well-designed, representative population-based surveillance in primary and secondary care to monitor trends in transmission and severe disease. Where possible, all SARS-CoV-2-positive specimens from representative surveillance systems should be sequenced and reported to GISAID and/or TESSy to facilitate the assessment of circulating variants.
Vaccination
ECDC has provided interim public health considerations for COVID-19 vaccination roll-out during 2023 [20]. Since then, National Technical Immunisation Groups (NITAGs) in several EU/EEA countries have issued recommendations regarding the COVID-19 vaccination campaigns in autumn 2023. For most of the countries, target groups include: older adults (different age cut-offs, i.e. 50, 60, 65 years), individuals with underlying medical conditions regardless of age (including the immunocompromised), pregnant women, and healthcare workers. Recently, the WHO Regional Office for Europe (WHO/Europe) issued a guidance document on the development of national COVID-19 vaccination policies and planning, implementing, and monitoring integration of COVID-19 vaccination into national immunisation programmes (NIPs) [21].
Due to the evolving COVID-19 epidemiology, adherence to vaccination schedule is essential to protect people at high risk for severe disease and death. Countries should assess their readiness to identify target groups and conduct timely COVID-19 vaccination campaigns. Decisions made at the country level depend on several key evolving factors, such as the specific national epidemiological situation, availability of vaccines, projected vaccine uptake in different target groups, the capacity of healthcare systems to deliver vaccinations, and other factors. Communication campaigns aimed at the public and healthcare professionals are deemed necessary in an effort to reach high-risk groups and inform them of the importance to stay up to date with vaccination.
Consulted experts (in alphabetical order)
Erik Alm, Jon Bilbatua, Kim Brolin, Nick Bundle, Priyanka Nannapaneni, Ajibola Omokanye, Giulia Perego, Adriana Romani, Theodora Stavrou
References
- Ayijiang Y, Weiliang S, Jing W, Fanchong J, Yuanling Y, Xiaosu C, et al. Repeated Omicron infection alleviates SARS-CoV-2 immune imprinting. bioRxiv. 2023:2023.05.01.538516. Available at: http://biorxiv.org/content/early/2023/05/03/2023.05.01.538516.abstract
- European Centre for Disease Prevention and Control. SARS-CoV-2 variants of concern as of 10 August 2023. 2023 10 August 2023 Available at: https://www.ecdc.europa.eu/en/covid-19/variants-concern
- European Centre for Disease Prevention and Control. ECDC SARS-CoV-2 variant classification criteria and recommended EU/EEA Member State actions. Stockholm2023. Available at: https://www.ecdc.europa.eu/sites/default/files/documents/ECDC%20SARS-CoV-2%20variant%20classification%20criteria%20and%20recommended%20Member%20State%20actions.pdf
- World Health Organization. EG.5 Initial Risk Evaluation, 9 August 2023. 2023 09 August 2023 Available at: www.who.int/docs/default-source/coronaviruse/09082023eg.5_ire_final.pdf?sfvrsn=2aa2daee_1
- UKHSA Genomics Public Health Analysis Team UIDMT. SARS-CoV-2 genome sequence prevalence and growth rate update: 2 August 2023. 2023 02 August 2023 Available at: https://www.gov.uk/government/publications/sars-cov-2-genome-sequence-prevalence-and-growth-rate/sars-cov-2-genome-sequence-prevalence-and-growth-rate-update-2-august-2023#variant-declaration-v-23jul-01-eg51
- covSPECTRUM. EG.5* (Nextclade). 2023. Available at: https://cov-spectrum.org/explore/world/AllSamples/Past6M/variants?nextcladePangoLineage=EG.5*&
- covSPECTRUM. FL.1.5.1* (Nextclade). 2023 Available at: https://cov-spectrum.org/explore/world/AllSamples/Past6M/variants?nextcladePangoLineage=FL.1.5.1*&
- covSPECTRUM. XBB.1.16.6* (Nextclade). 2023 Available at: https://cov-spectrum.org/explore/world/AllSamples/Past6M/variants?nextcladePangoLineage=XBB.1.16.6*&
- World Health Organization. Weekly epidemiological update on COVID-19 - 10 August 2023. Geneva2023. Available at: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---10-august-2023
- Government of Ireland. Ireland's COVID-19 Data Hub - National Statistics, Information & Data. 2023. Available at: https://covid19ireland-geohive.hub.arcgis.com/
- Magri G. Noticed many people getting sick this summer? GPs have too. Times Malta. 10 Augusta 2023 2023. Available at: https://timesofmalta.com/articles/view/gps-report-rise-covid19-cases-respiratory-infections.1048990
- Inácio AM. Casos de Covid-19 triplicaram na última semana em Portugal, mas sem gravidade. Diario de noticias. 15 August 2023 2023.
- Japan sees increase in COVID cases for 17 straight weeks. NKH World Japan. 04 August 2023 2023.
- Boram K. S. Korea's weekly virus cases rise for 7 straight weeks, but pace slows down. YONHAP News Agency. 16 August 2023 2023. Available at: https://en.yna.co.kr/view/AEN20230816005800320
- Fiorillo C. Covid-19 cases up 24% in England as number of Brits in hospital increase. Mirror. 28 July 2023 2023. Available at: https://www.mirror.co.uk/news/uk-news/covid-19-cases-up-24-30568367
- Centers for Disease Control and Prevention. COVID Data Tracker. CDC; 2023. Available at: https://covid.cdc.gov/covid-data-tracker/#datatracker-home
- Centers for Disease Control and Prevention. COVID Data Tracker - Variant Proportion. CDC; 2023. Available at: https://covid.cdc.gov/covid-data-tracker/#variant-proportions
- Mordoh H. New COVID-19 variant EG.5 is on the rise, dominant in the US. WISHTVCOM. 16 August 2023 2023. Available at: https://www.wishtv.com/news/national/new-covid-19-variant-eg-5-is-on-the-rise-dominant-in-the-us/
- European Centre for Disease Prevention and Control. Country overview report: week 31 2023. Stockholm2023. Available at: https://covid19-country-overviews.ecdc.europa.eu/index.html
- European Centre for Disease Prevention and Control. Interim public health considerations for COVID-19 vaccination roll-out during 2023. Stockholm 2023. Available at: https://www.ecdc.europa.eu/en/publications-data/interim-public-health-considerations-covid-19-vaccination-roll-out-during-2023
- World Health Organization Regional Office for Europe. Guidance on developing national COVID-19 vaccination policy and integrating COVID-19 vaccination into national immunization programmes and broader health care delivery mechanisms in the WHO European Region: August 2023. 2023 02 August 2023 Available at: https://www.who.int/europe/publications/i/item/WHO-EURO-2023-7892-47660-70230”


Share this page