Cholera worldwide overview
Monthly update as of 22 June 2026
Since 26 May 2026 and as of 22 June 2026, 19 659 new cholera cases, including 261 new deaths, have been reported worldwide.
New cases have been reported from Afghanistan, Angola, Burundi, Congo, Democratic Republic of The Congo, Haiti, India, Kenya, Malawi, Mozambique, Nigeria, Pakistan, Yemen and Zambia.
The five countries reporting most cases are Nigeria (8 051), the Democratic Republic of the Congo (DRC) (7 923), Angola (1 930), Malawi (882), and Burundi (358).
New deaths have been reported from Afghanistan, Angola, Burundi, Congo, DRC, Haiti, Mozambique, Nigeria, and Yemen.
The five countries reporting most new deaths are DRC (112), Nigeria (77), Angola (42), Congo (27), and Mozambique (2).
In addition, 17 405 new cases were reported or collected retrospectively from before 26 May 2026.
In the previous reporting period (28 April to 26 May 2026), 3 596 new cholera cases, including 176 new deaths, were reported worldwide.
Since 1 January 2026 and as of 22 June 2026, 105 813 cholera cases, including 1 216 deaths, have been reported worldwide.
In comparison, since 1 January 2025 and as of 22 June 2025, 121 736 cholera cases, including 1 576 deaths, were reported worldwide.
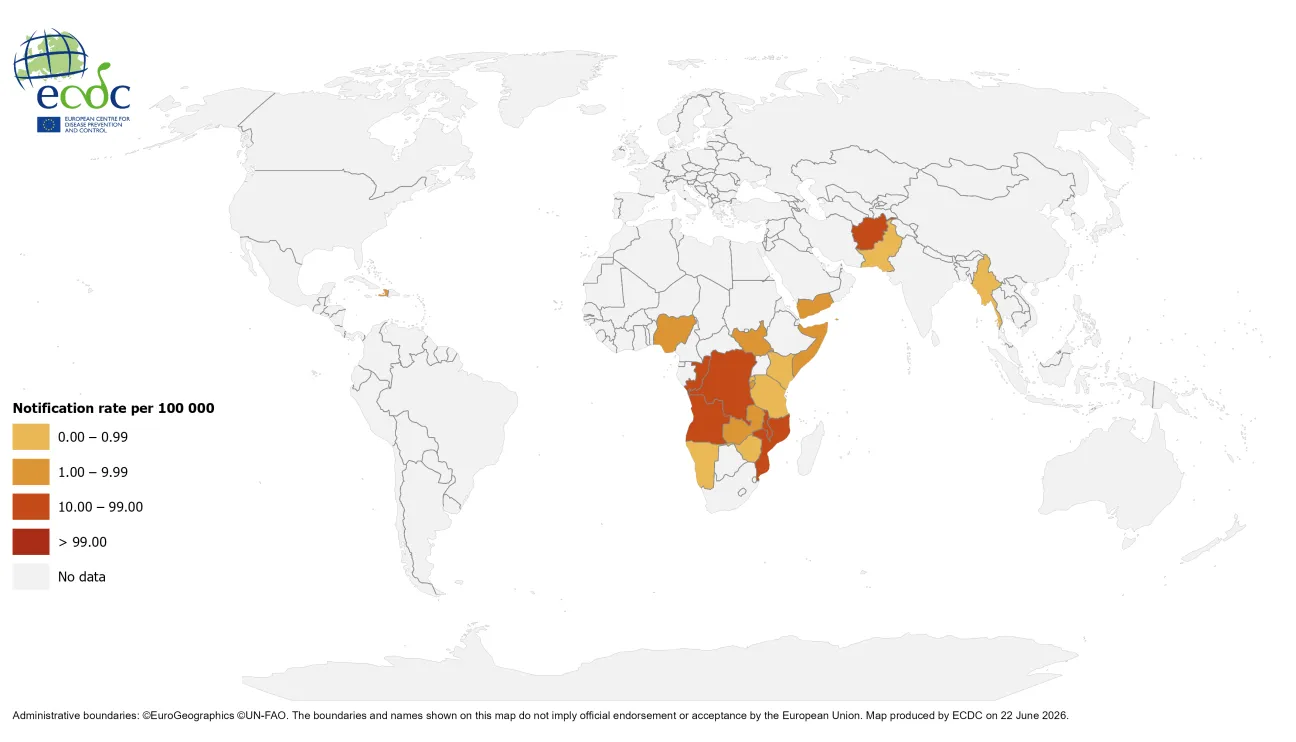
Geographical distribution of cholera cases reported worldwide from April to June 2026
Update
Since the last update, new cases and new deaths have been reported from:
Asia
Afghanistan: Since 13 April 2026 and as of 18 May 2026, 15 421 new cases, including nine new deaths, have been reported. Since 1 January 2026 and as of 18 May 2026, 40 085 cases, including 16 deaths, have been reported. In comparison, in 2025 and as of 17 March 2025, 19 652 cases, including eight deaths, were reported.
India: Since 9 February 2026 and as of 9 March 2026, 10 new cases have been reported. Since 1 January 2026 and as of 09 March 2026, 36 cases have been reported. In comparison, in 2025 and as of 28 April 2025, 440 cases were reported.
Pakistan: Since 16 March 2026 and as of 20 April 2026, 957 new cases have been reported. Since 1 January 2026 and as of 20 April 2026, 2 604 cases have been reported. In comparison, in 2025 and as of 19 May 2025, 11 181 cases were reported.
Yemen: Since 6 April 2026 and as of 4 May 2026, 872 new cases, including three new deaths, have been reported. Since 1 January 2026 and as of 4 May 2026, 4 358 cases, including six deaths, have been reported. In comparison, in 2025 and as of 24 February 2025, 10 080 cases, including 10 deaths, were reported.
Since 26 May 2026, no updates have been reported by: Myanmar/Burma.
In addition, on 23 June 2026, Taiwan Centers for Disease Control reported a locally-acquired case of cholera in a woman in her 70s with no recent travel history. The patient developed diarrhea, vomiting and convulsions in early June and was later hospitalised when her condition worsened.
Samples from the patient tested positive to Vibrio cholerae O1 (Hikojima serotype). The patient was hospitalised and, following treatment, her condition improved and she was discharged. Taiwan has reported single locally-acquired cases of cholera in 2020, 2022 and 2023.
Africa
Angola: Since 10 May 2026 and as of 14 June 2026, 1 930 new cases, including 42 new deaths, have been reported. Since 1 January 2026 and as of 14 June 2026, 5 076 cases, including 104 deaths, have been reported. In comparison, in 2025 and as of 30 April 2025, 14 090 cases, including 505 deaths, were reported.
Burundi: Since 10 May 2026 and as of 14 June 2026, 358 new cases, including one new death, has been reported. Since 01 January 2026 and as of 14 June 2026, 1 373 cases, including three deaths have been reported. In comparison, in 2025 and as of 17 March 2025, 129 cases were reported.
Congo: Since 10 May 2026 and as of 14 June 2026, 298 new cases, including 27 new deaths, have been reported. Since 1 January 2026 and as of 14 June 2026, 689 cases, including 60 deaths, have been reported. In comparison, in 2025 and as of 22 June 2025, no cases were reported.
Democratic Republic of The Congo: Since 10 May 2026 and as of 14 June 2026, 7 923 new cases, including 112 new deaths, have been reported. Since 1 January 2026 and as of 14 June 2026, 29 341 cases, including 838 deaths, have been reported. In comparison, in 2025 and as of 10 March 2025, 11 918 cases, including 240 deaths, were reported.
Kenya: Since 31 December 2025 and as of 14 June 2026, 37 new cases have been reported. Since 1 January 2026 and as of 14 June 2026, 37 cases have been reported. In comparison, in 2025 and as of 30 April 2025, 125 cases, including six deaths, were reported.
Malawi: Since 10 May 2026 and as of 14 June 2026, 882 new cases have been reported. Since 1 January 2026 and as of 14 June 2026, 2 615 cases, including five deaths, have been reported. In comparison, in 2025 and as of 7 April 2025, 91 cases, including three deaths, were reported.
Mozambique: Since 10 May 2026 and as of 14 June 2026, 170 new cases, including two new deaths, have been reported. Since 1 January 2026 and as of 14 June 2026, 7 186 cases, including 61 deaths, have been reported. In comparison, in 2025 and as of 30 April 2025, 2 851 cases, including 29 deaths, were reported.
Nigeria: Since 10 May 2026 and as of 14 June 2026, 8 051 new cases, including 77 new deaths, have been reported. Since 1 January 2026 and as of 14 June 2026, 8 994 cases, including 96 deaths, have been reported. In comparison, in 2025 and as of 17 March 2025, 1 214 cases, including 28 deaths, were reported.
Zambia: Since 10 May 2026 and as of 14 June 2026, 10 new cases have been reported. Since 1 January 2026 and as of 14 June 2026, 997 cases, including 16 deaths, have been reported. In comparison, in 2025 and as of 15 April 2025, 463 cases, including nine deaths, were reported.
Since 26 May 2026, no updates have been reported by: Ethiopia, Namibia, Rwanda, Somalia, South Sudan, Sudan, United Republic of Tanzania, or Zimbabwe.
Americas
Haiti: Since 16 February 2026 and as of 06 April 2026, 145 new cases have been reported. One death previously reported in Haiti has been retrospectively removed. Since 1 January 2026 and as of 6 April 2026, 357 cases, including one death, has been reported. In comparison, in 2025 and as of 26 May 2025, 1 879 cases, including 31 deaths, were reported.
ECDC assessment
Cholera cases have continued to be reported in Africa and Asia, the Middle East, and the Americas.
In this context, although the likelihood of cholera infection for travellers visiting these countries remains low, sporadic importation of cases to the EU/EEA is possible.
In the EU/EEA, cholera is rare and primarily associated with travel to endemic countries. Since 2025, only events of locally acquired cholera cases are reported at the EU/EEA level; however, imported and locally acquired cholera cases are reported to the World Health Organization (WHO) on an annual basis. In 2024, 16 imported cases were reported by eight EU/EEA countries, while 12 were reported in 2023, 29 in 2022, two in 2021, and none in 2020. In 2019, 25 cases were reported in EU/EEA countries (including the United Kingdom). All cases had a travel history to cholera-affected areas.
Vaccination should be considered for travellers at higher risk of infection, such as emergency and relief workers who may be directly exposed. Vaccination is generally not recommended for other travellers. Travellers to cholera-endemic areas should seek advice from travel health clinics to assess their personal risk, and apply precautionary sanitary and hygiene measures to prevent infection. Such measures can include drinking bottled water or water treated with chlorine, carefully washing fruit and vegetables with bottled or chlorinated water before consumption, regularly washing hands with soap, eating thoroughly cooked food, and avoiding the consumption of raw seafood products.
Actions
ECDC continues to monitor cholera outbreaks globally through its epidemic intelligence activities in order to identify significant changes in epidemiology and provide timely updates to public health authorities.
Reports are published on a monthly basis. The worldwide overview of cholera outbreaks is available on ECDC's website.
Read more
All updates on cholera

Cholera is an acute diarrhoeal infection caused by the bacterium Vibrio cholera of serogroups O1 or O139. Humans are the only relevant reservoir, even though Vibrios can survive for a long time in coastal waters contaminated by human excreta.