Epidemiological update: hepatitis A outbreak in the EU/EEA mostly affecting men who have sex with menArchived
Since the last epidemiological update on this multi-country hepatitis A outbreak published on 22 December 2017, 22 EU/EEA countries (Austria, Belgium, Croatia, the Czech Republic, Denmark, Estonia, Finland, France, Germany, Greece, Ireland, Italy, Latvia, Luxembourg, Malta, the Netherlands, Norway, Portugal, Slovenia, Spain, Sweden and the United Kingdom-England) have reported 320 new outbreak-confirmed cases. The outbreak-confirmed cases are EU/EEA residents with laboratory-confirmed hepatitis A virus (HAV) genotype IA and a sequence with ≥99.3% homology to one of the three HAV genotype IA outbreak strains (VRD_521_2016; RIVM-HAV16-090; and V16-25801) based on overlapping fragments at the VP1-2a region.
As of 19 March 2018, the number of outbreak-confirmed cases reported in the 22 EU/EEA countries since 1 June 2016 is 4 101 (Figure 1). For 3 873 of these cases, information on gender is available, with a male-to-female (M/F) ratio of 7.2, a sharp reduction from the M/F ratio has been observed since May when it was 12.7. No other strains were reported to be widely circulating among men who have sex with men (MSM) apart from the three outbreak strains and their close variants, which are captured in Figure 1.
Figure 1. Distribution of hepatitis A outbreak-confirmed cases, by month of onset and genetic sequence, June 2016 to February 2018, as of 19 March 2018, EU/EEA (n=4 101)
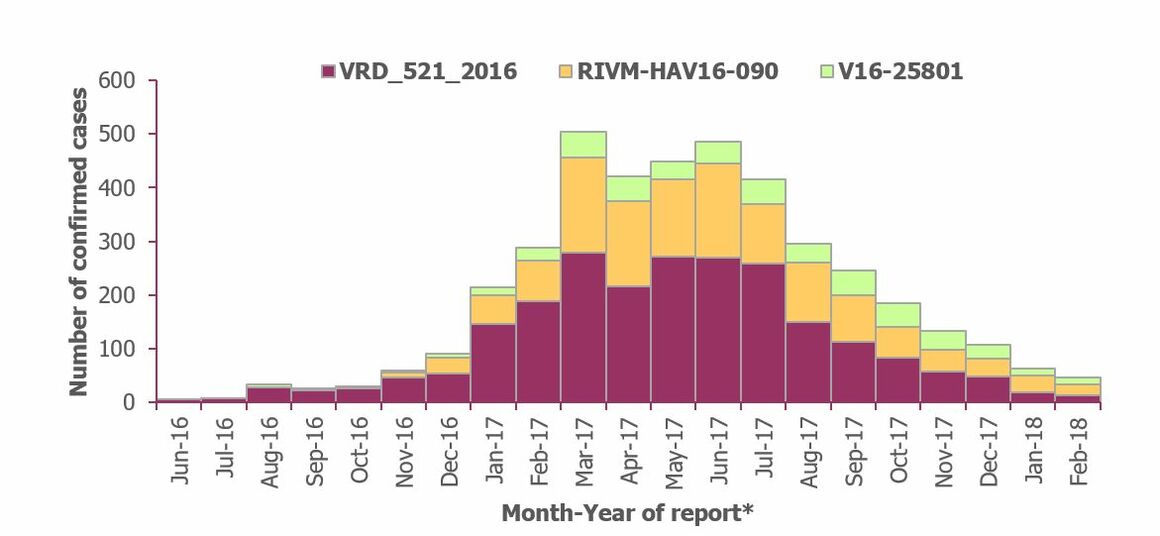
Countries included: Austria (until November 2017), Belgium, Croatia, the Czech Republic, Denmark, Estonia, Finland (until November 2017), France, Germany, Greece, Ireland, Italy, Latvia, Luxembourg (until November 2017), Malta, the Netherlands, Norway, Portugal, Slovenia, Spain, Sweden and the United Kingdom-England.
March 2017 was the month with the largest number of outbreak-confirmed cases (504). There may be substantial reporting delays (weeks or even months) in sequencing information and the number of cases with onset in more recent months is likely to increase once more sequencing results are available. However, the month of the outbreak peak, March 2017, and the following plateau, from April to July 2017, are unlikely to change.
Outbreak-confirmed cases provide an underestimation of the true extent of the outbreak. This is because sequencing information is only available for a proportion of hepatitis A cases as sampling strategies vary widely from country to country, and during the different phases of the outbreak. Between January 2017 and February 2018, 4 742 (28%) of the 17 210 laboratory-confirmed hepatitis A case strains in 21 EU/EEA countries (Austria, Belgium, Croatia, Denmark, Estonia, France, Germany, Greece, Finland, Ireland, Italy, Latvia, Luxembourg, Malta, the Netherlands, Norway, Portugal, Slovenia, Spain, Sweden and the United Kingdom-England) were sequenced. Of these, 4 742 sequenced cases, 3 924 (84%) were infected with one of the three outbreak strains.
In order to better define the extent of this outbreak, we describe all hepatitis A laboratory-confirmed cases, with or without information on genetic sequence, and the related male-to-female ratio. From January 2017 to February 2018, 26 countries (the 22 mentioned above, plus Hungary, Iceland, Lithuania and Poland) reported 21 230 laboratory-confirmed cases with an overall M/F gender ratio of 3.3. The M/F ratio from January to December 2017 was 3.5 and from January 2018 to February 2018 1.7. The highest M/F ratio was 4.9, reported in May 2017. Since then, the number of male cases decreased progressively until February 2018 when the M/F ratio was 1.8 (Figure 2).
The 20 089 hepatitis A cases reported by the 26 countries from January to December 2017 represent an almost four-fold increase compared with the average 5 648 cases reported for the same period between 2012 and 2015. 2016 was excluded from the comparison as the current outbreak was already underway at the time.
Of these, information on gender is available for 20 067 cases: 15 591 males and 4 476 females. Compared with the average number of hepatitis A cases reported during the same period between 2012 and 2015, the number of male cases increased by 413% and the number of female cases increased by 70%.
Figure 2. Distribution of hepatitis A cases by gender and male-to-female ratio, January 2012 to March 2018, as of 19 March 2018, EU/EEA
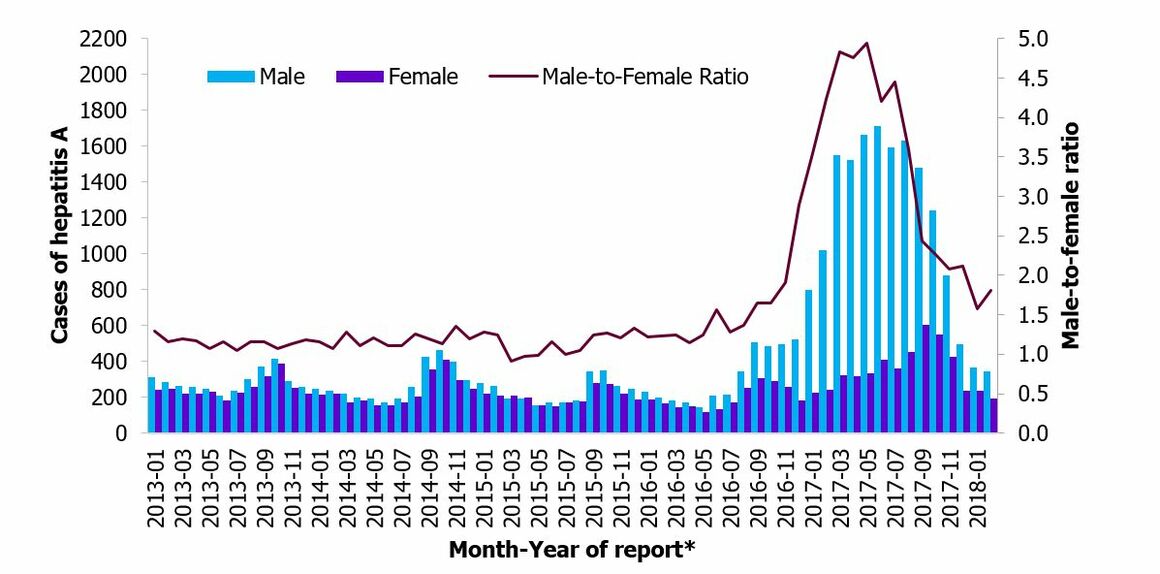
Countries included: Austria, Belgium, the Czech Republic, Denmark, Croatia, Estonia, Finland, France, Hungary, Germany, Greece, Ireland, Iceland, Italy, Latvia, Lithuania, Luxembourg, Malta, the Netherlands, Norway, Poland, Portugal, Slovenia, Spain, Sweden and the United Kingdom. The 2017–2018 data from the United Kingdom are only for England. Data from Belgium are missing for 2015 and 2016. Data from Austria, Czech Republic and Luxembourg include cases reported only until November 2017. Data from Poland include cases reported only until December 2017
Slovakia did not report cases in 2017 for this epidemiological update, but ECDC epidemic intelligence screening identified 127 hepatitis A cases in the country between November 2017 and January 2018. In 2017, Slovakia identified 672 cases compared with 1 157 cases during the same period in 2016, which is a two-fold decrease. In Poland Romania and Slovakia, no cases could be linked to the current outbreak since sequencing information was not available.
ECDC asked EU/EEA countries to report on events that could contribute to the spread of the outbreak strains in population groups at increased risk of infection or in the community. As a result of these spill-over events, a limited increase has been noted in females, children and the elderly in parallel with the large increase in male cases. In previous updates, Austria, France, Italy and the Netherlands reported an increase in females to a greater or lesser extent. In the Netherlands 33% of hepatitis A cases in females were infected with one of the outbreak strains. The Czech Republic, France and Italy reported an increase in children, and France and Italy also reported an increase, but in the elderly. Germany reported a small food-borne outbreak of hepatitis A involving a food-handler. Since the last epidemiological update, UK-England reported an increase in females, and
in Portugal a cluster of 15 hepatitis A cases among Roma population was identified. In this cluster, two of the cases were sequenced and found to be infected with one of the VRD_521_2016 outbreak strain.
Publications describing the characteristics of cases in Denmark, France, Germany, Malta, the Netherlands, Spain and UK are available online.
Vaccination
The main prevention measure in this context is hepatitis A vaccination of MSM and their close contacts. Hepatitis A vaccine availability in the EU is currently limited, with some countries reporting shortages to a lesser or greater extent, including, the Czech Republic, Denmark, France, Germany, Italy, Malta, Norway, Spain, and since the last update, also the United Kingdom. On the other hand, Austria, Belgium, Croatia, Estonia, Finland, Greece, Hungary, Iceland, Ireland, Latvia, Lithuania, Luxembourg, the Netherlands, Portugal, Slovenia and Sweden reported no, or no longer, shortages.
It is suggested that vaccination can be promoted and offered to MSM attending Pride festivals, where there may be an increased likelihood of contact with hepatitis A-infected individuals. However, limited hepatitis A vaccine availability in some countries may hinder the implementation of these measures.
Since the last ECDC rapid risk assessment in June 2017, Austria, Denmark, France, Germany, Italy, Norway, Portugal, Spain and the United Kingdom have issued new vaccination recommendations.
Assessment
Between June 2016 and November 2017, 22 EU/EEA countries reported 4 101 hepatitis A outbreak-confirmed cases associated with this outbreak that peaked in March 2017. The number of outbreak-confirmed cases and their distribution in time describes the dynamic of the outbreak, but is also influenced by the different countries’ sequencing strategies. However, the time of the outbreak peak, the plateau from April to July 2017 and the following decrease are not expected to change.
In addition, since January 2017, 21 230 hepatitis A laboratory-confirmed cases were notified by 26 EU/EEA countries. The number of laboratory-confirmed cases peaked in June 2017, while the highest M/F ratio was observed in May 2017. As of 19 March 2018, the monthly number of laboratory-confirmed cases, although still higher than in previous years, was returning to baseline. The M/F ratio has also strongly decreased in recent months although remaining higher than in previous years.
Since 2017, a considerable increase in the total number of hepatitis A cases in women has also been observed, with outbreak strains circulating in this group too. Furthermore, this is the first time that a cluster of cases involving one of the outbreak strains has been identified in the Roma population. This indicates that the outbreak has spilled over to the non-MSM population and to population groups at increased risk of infection.
Although decreasing in its intensity, the outbreak is still ongoing and more cases associated with this event are to be expected in EU/EEA countries in the coming months.
The conclusions and options for response set out in ECDC’s rapid risk assessment entitled ‘Hepatitis A outbreak in the EU/EEA mostly affecting men who have sex with men – Third update, 28 June 2017’, remain valid.


